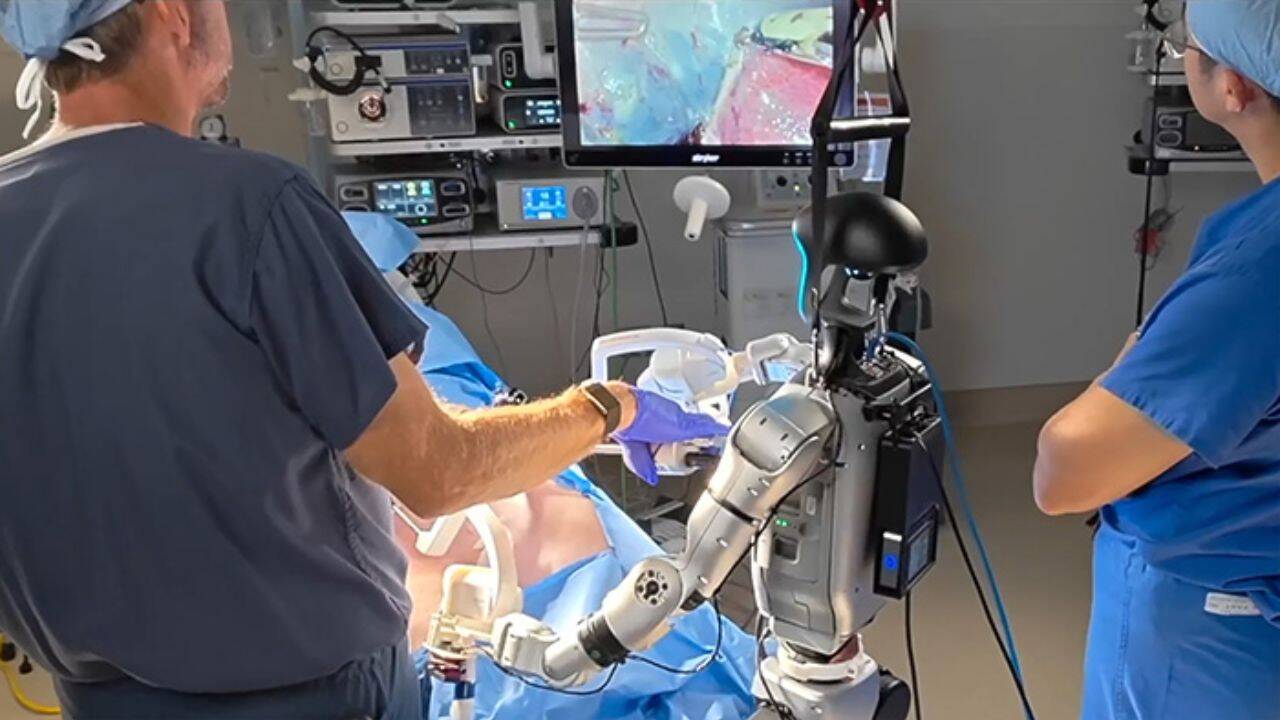
The traditional surgical robotics sector relies on heavy, fixed-infrastructure capital assets that restrict advanced care to highly capitalized urban trauma centers. The publication of the University of California San Diego (UCSD) preclinical study in Nature, titled "In vivo feasibility study of humanoid robots in surgery," alters the economic and operational trajectory of medical automation. By using a 5-foot-tall, 60-pound general-purpose humanoid platform nicknamed "Surgie" to execute cholecystectomies (gallbladder removals) on live non-primate mammals, researchers demonstrated that general-purpose anthropomorphic kinematics can achieve the localized precision required for minimally invasive procedures. This shift decouples advanced surgical execution from specialized, single-use hardware ecosystems.
Understanding the implications of this validation requires moving past the superficial framing of a "medical breakthrough" to analyze the underlying kinematic frameworks, control loops, and economic trade-offs that dictate the viability of humanoid field medicine.
The Architectural Divergence: Task-Specific vs. General-Purpose Kinematics
Current clinical standards for robotic surgery are defined by platforms like the Intuitive Surgical da Vinci system. These platforms utilize a fixed-base architecture weighing approximately 1,800 pounds, requiring dedicated operating rooms, structural retrofitting, and proprietary end-effectors. The architectural divergence introduced by the UCSD research team centers on form factor utility and structural footprint.
Kinematic Constraints and Form Factors
| Engineering Metric | Specialized Surgical Platforms (e.g., da Vinci) | Anthropomorphic Humanoid Systems (Surgie) |
|---|---|---|
| System Mass | ~1,800 lbs | 60 lbs |
| Form Factor | Multi-arm fixed gantry, multi-quadrant overhead boom | 5-foot-tall bimanual mobile biped/torso |
| End-Effectors | Proprietary, micro-wristed digital instruments | Custom adapters holding standard laparoscopic tools |
| Degrees of Freedom (DoF) | Optimized strictly for intracorporeal triangulation | Human-mimetic anthropomorphic workspace arm/wrist linkages |
| Spatial Footprint | Stationary, occupying a permanent surgical bay quadrant | Mobile, variable position, matching human assistant footprint |
Specialized surgical platforms maximize mechanical rigidity. By anchoring multiple independent arms to a heavy central column, these systems eliminate high-frequency structural vibrations and minimize geometric error propagation. The end-effectors use specialized pulley-driven wristed mechanisms that map human wrist movements to sub-centimeter spaces inside the patient's body.
The Surgie platform uses a completely different mechanical strategy. It utilizes a lightweight, compliant bimanual structural design intended to replicate human anatomical dimensions. The core challenge here is that general-purpose humanoid arms exhibit lower structural stiffness than fixed industrial gantries. Lower stiffness increases the system's susceptibility to deflection when external forces are applied during tissue retraction.
To overcome this structural limitation without modifying the robot's physical frame, the UCSD engineering team built physical tool adapters. These adapters secured standard, manual laparoscopic instruments directly to the humanoid's end-effectors, demonstrating that specialized, proprietary instruments are no longer a strict prerequisite for high-precision digital surgery.
The Control Loop Bottleneck: Teleoperation, Latency, and Recalibration Dynamics
The UCSD preclinical trials evaluated two distinct configurations in live animal models: a human-robot hybrid team (one humanoid acting alongside a human surgical assistant) and a dual-robot team (two humanoid units working side by side, each controlling a separate surgical tool). While both configurations successfully completed the cholecystectomy procedures, the operational execution revealed significant bottlenecks within the bilateral teleoperation control loop.
[Human Surgeon Console] ---> (Control Input Data) ---> [Network Interface / Latency]
|
v
[Mechanical Deflection] <--- (Recalibration Loop) <--- [Surgie Humanoid Actuators]
The first operational limitation is systemic mechanical drift. During the live procedures, the humanoid robots required multiple intraoperative recalibrations. As the robots performed repeated, high-precision actions through fixed laparoscopic entry ports (trocars), small mechanical discrepancies accumulated in the joint actuators. This required the surgical team to repeatedly pause the procedure to re-align the digital control coordinates with the physical space of the operating table.
This drift directly impacts total procedure time. While a modern manual or specialized robotic cholecystectomy typically takes 30 to 45 minutes, the humanoid-led procedures took significantly longer. This variance is not a structural failure of the concept; it mirrors the early developmental phase of laparoscopic automation. When specialized robotic laparoscopic surgery was introduced, initial procedure times regularly exceeded six hours before optimization brought them down to contemporary standards.
The second operational bottleneck is command propagation latency. In a local teleoperation setup, the delay between the human surgeon moving the input console and the humanoid executing that movement is negligible. However, expanding this architecture to rural clinics, battlefield triages, or forward operating bases introduces network-induced transport latency.
When teleoperating over long distances, round-trip times exceeding 100 milliseconds degrade a surgeon’s tactile feedback and spatial awareness. This latency increases the risk of accidental tissue perforation during high-stakes maneuvers like cystic artery dissection.
The Three Pillars of Surgical Humanoid Autonomy
Achieving operational viability outside of controlled preclinical research centers requires moving beyond continuous direct human control. True utility depends on transitioning the humanoid from a pure teleoperated puppet to an agent capable of variable autonomy. This transition relies on three distinct technological pillars:
- Contextual Computer Vision and Semantic Segmentation: The robot's onboard camera arrays must process low-latency video feeds to distinguish between liver tissue, gallbladder boundaries, and critical vascular structures. This requires deploying deep-learning vision models optimized for real-time anatomical tracking despite fluid obstructions or smoke from electrocautery tools.
- Dynamic Task-Space Constraints (Virtual Fixturing): To prevent human operators or autonomous path-planning algorithms from damaging healthy tissue, software control loops must enforce virtual boundaries. These software barriers dynamically restrict the robot's end-effectors from entering critical, user-defined spatial zones, creating an digital safety buffer around major blood vessels.
- Behavioral Cloning and Contact-Rich Action Primitives: Humanoids must automate low-risk, repetitive sub-tasks such as camera positioning, wound irrigation, tool retrieval, and post-operative waste management. By offloading these administrative physical tasks to an autonomous assistant, the cognitive load on the primary surgeon is vastly reduced.
Economic Viability and Field Deployment Constraints
The primary driver for implementing humanoid architectures in medicine is not superior mechanical precision compared to specialized systems; it is the economics of general-purpose utility.
Specialized surgical platforms represent an immense capital expenditure, often costing between $1.5 million and $2.5 million per unit, plus substantial annual maintenance contracts. This high cost creates a steep financial barrier that prevents rural health networks and developing economies from adopting the technology.
Humanoid platforms, by contrast, are engineered for mass production across multiple industrial sectors. By leveraging supply chains optimized for logistics, manufacturing, and general service industries, the hardware cost of a humanoid frame is orders of magnitude lower.
Furthermore, a specialized surgical robot sits idle when no surgeries are scheduled. A humanoid platform like Surgie can transition between active surgical execution, preoperative room preparation, tool sterilization, and postoperative environmental cleaning. This multi-role utility reconfigures the amortization model of clinical robotics, shifting the asset from a single-use cost center to an adaptable utility platform.
However, moving these platforms into austere environments introduces distinct field liabilities:
- Kinematic Port Restrictions: Operating through a tiny incision requires the robot's arm joints to pivot precisely around a fixed point in space (the remote center of motion). If the humanoid's base shifts slightly on an uneven floor, the tool shaft can bind within the incision, risking severe internal tissue tearing.
- Environmental Integrity Deficits: Current humanoid designs are susceptible to particulate ingress and fluid exposure. Standard operating procedures require rigorous chemical sterilization or complete sterile bagging of the entire mechanical frame to prevent cross-contamination in the sterile field.
- Power Density Constraints: Continuous high-torque actuation across 20+ degrees of freedom drains onboard battery systems quickly. This limits untethered field operations to short windows unless the unit is attached to a continuous external power supply, which compromises its mobility advantages in disaster zones.
The Tactical Roadmap for Clinical Integration
The path toward deploying general-purpose humanoids in human clinical environments requires a phased, risk-mitigated integration strategy rather than an immediate replacement of existing infrastructure.
Phase 1: Environmental Logistics (Sterilization, Tool Fetching)
│
▼
Phase 2: Active Co-Assistance (Camera Holding, Tissue Retraction)
│
▼
Phase 3: Teleoperated Execution (Remote Specialist Interventions)
The first phase limits humanoid deployment entirely to non-contact environmental logistics. Humanoids should be integrated into the operating room to handle sterile tool delivery, manage waste disposal, and execute post-operative cleanup protocols. This phase validates the robot's navigation reliability and safety profiles around human staff without introducing any risk to the patient.
The second phase introduces active co-assistance during live procedures. The humanoid takes over stable, repetitive tasks that typically strain human assistants, such as maintaining static retraction on the liver or holding laparoscopic camera arrays steady for extended periods. The robot operates under the direct visual supervision of a primary surgeon who can instantly override the machine’s physical actuators if needed.
The third phase implements teleoperated surgical execution in localized, underserved regions. Specialist surgeons based at central teaching hospitals can utilize low-latency network connections to control field-deployed humanoids in rural clinics or emergency transport vehicles.
By prioritizing robust, localized teleoperation platforms that function reliably despite network disruptions, healthcare networks can scale specialized trauma care to remote areas well before fully autonomous surgical artificial intelligence receives regulatory clearance.